Introduction
Though not well publicized, back pain is one of the major public health crises facing the Unites States today. Back pain is the most common cause of loss of work. Back and spinal problems now are the 2nd leading cause of disability in the U.S. Worldwide, back pain causes more disability than any other condition. In other words, you are more likely to become disabled from back pain than you are from heart disease, stroke or cancer. Almost everyone knows someone with a severe back condition. It’s no surprise then that studies show that 70% of Americans will suffer from significant back pain at some point in their lives. On a yearly basis 15%-20% of Americans will be afflicted. If you suffer from significant back pain there are odds that you will continue to be plagued by pain for some time. The majority of Americans afflicted with back pain don’t recover quickly. Studies show that a third of Americans recover within one month, a third within 2-5 months and a third take >6 months to recover. When you do recover it’s not always over. It’s estimated that 50% of people with a prior episode of back pain will have a recurrent episode by one year, 60% by 2 years and 70% by 5 years.
Since lower back pain is such an important public health issue that effects many of us, it’s important to understand as much as we can about this disease so we can navigate through our own health care and better understand what’s going on in our bodies. There are several different causes of back pain. The most common cause of back pain is also the most benign. Sprains and strains are injuries to the tendons, muscles and ligaments of the spine. The intervertebral disc, a cushion between the bony vertebrae of the spine, can cause back pain in 20%-50% of us. A disc can cause pain in several ways. A herniated disc occurs when the center of a disc protrudes through its lining. A degenerated disc occurs either through wear and tear or after disc injury. Another common cause of back pain is the facet joint, resulting in a facet joint syndrome. This is the joint that lies behind the disc and joins vertebra together. This is the cause of back pain in 15%-45% of us. The sacroiliac joint is a paired joint that joins the pelvis and spine together. Sacroiliac joint pain can develop over time, usually from being overly stressed. This results in a wear and tear, or arthritis, of the joint. Spinal stenosis is a condition that occurs when there is a narrowing of the normal passageways of the spine, intruding on the nerves that travel up and down the spine. Spondylolisthesis occurs when the vertebra slip past one another instead of being normally aligned. Spondylolisthesis causes back pain when there is abnormal motion between vertebrae or when the slippage has become so great that there is compression of the nerves of the spine. Lastly, one cannot ignore failed back surgery syndrome (FBSS). FBSS occurs when pain persists, or even gets worse, after a spine surgery that was performed to treat back pain in the first place.
Sprains and Strains
Discussion
Sprains and strains involve injuries to ligaments, tendons or muscle. Ligaments connect bones to bones. In the spine they provide stability. Tendons connect muscles to bone. In the spine these muscles allow the spine to move and also result in stability by resisting abnormal movement. In a sprain there has been over-stretching of a ligament. In a strain there has been over-stretching of a tendon or its muscle. Sprains and strains are usually caused by accidents or are the result of over-use injuries. This can occur from violent and rapid motions, such as in a car accident, or can occur from over stressing tendons and ligaments during exercise or while playing sports. Most sprains and strains are low-grade, meaning that they result in stretching and shearing of tendons and ligaments without tearing them. The pain from these low-grade sprains and strains usually resolves within 6-8 weeks and responds quite well to physical therapy or chiropractic care. High grade strains involve partial or complete tearing of ligaments, muscles and tendons. These are usually the result of violent injuries and almost always require surgery to the spine. Even when a sprain/strain is low grade it can cause permanent damage. Over stretching of ligaments or tendons can be very like over stretching a rubber band. The ligaments or tendons can become floppy and lose elasticity without tearing. As a result, the injured ligaments or tendons will poorly resist abnormal forces in the future and may make it easier to reinjure the spine.
Symptoms:
- Involves upper, mid or low back
- Constant aching back pain
- Pain radiating to buttocks, hips or thighs
- Back stiffness
- Painful sleep
- Pain with exertion or physical activity
- Pain aggravation with range of motion of back (bending forwards, bending backwards, lateral bending)
Signs
- Back muscle tenderness
- Diminished range of motion (difficulty with normal motion)
- Feeling of taught and tender knots in muscle
Diagnosis
Time is the best way to diagnose a sprain or strain, since many more serious and permanent conditions have similar symptoms. When symptoms rapidly improve over time, usually 6-8 weeks, one can presume that most of the back pain was from sprains and strains. Usually there will be improvement with or without therapy, although therapy brings improvement more quickly. Also, since the major structures of the spine are unhurt an MRI will be normal or will show normal age related changes. X-rays may show muscle spasm resulting in a straightening of the normal spinal curves.
Treatment consists of the following conservative care measures:
- Non-steroidal anti-inflammatory medications (Like Advil, Motrin, Naprosyn)
- Muscle relaxants (Like Robaxin, Baclofen or Flexeril)
- Activity restrictions (No heavy lifting, bending, twisting or strenuous activity)
- Physical therapy
- Chiropractic care
- Home exercise therapy
Herniated Disc
A herniated disc is an injury to the disc that can cause back and/or extremity pain. In a herniated disc there is displacement of disc material beyond the normal confines of the disc.
Discussion
The disc lies between the bony vertebra of the spine. The disc is a cushiony structure consisting of a rough outer band and a soft inner core. In this sense the disc has been likened to a jelly doughnut. The outer band is made up of a tough fiber called collagen. The inner core is a gel like consistency, although it becomes fibrous with aging or degeneration. The disc has 2 functions; it cushions the spine and it stabilizes the spine. It does this by resisting abnormal motion and forces. Disc herniations are a form of injury to the disc and are a common cause of lower back pain, especially in younger patients. Disc herniations are not caused by degeneration nor are they caused by normal wear and tear. A disc herniation is always abnormal.
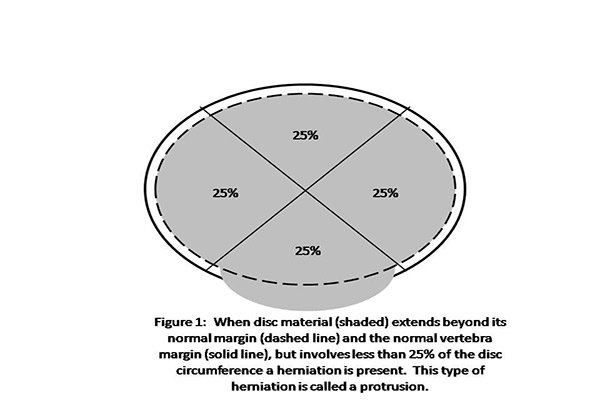
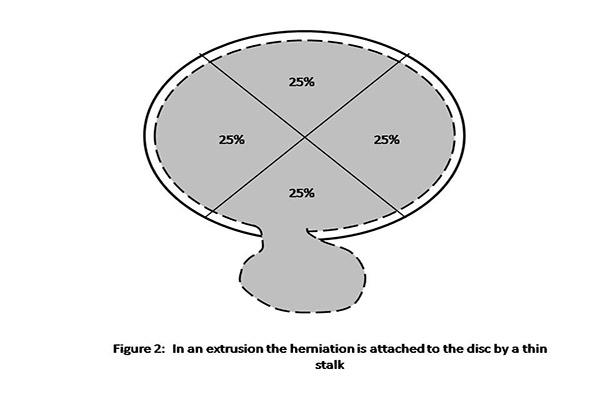
A disc herniation is defined as a localized displacement of disc material involving 25% or less of the disc circumference. Disc herniations can be further subdivided into protrusions and extrusions. In a protrusion the herniated disc material possesses a sizable connection to the disc space (Figure 1). In an extrusion a large amount of disc material has extended beyond the disc space, connected only by a thin stalk (Figure 2). In order for a herniation to occur, whether a protrusion or an extrusion, there has to be a tear in the fibrous band (called the annulus) surrounding the inner gel (called the nucleus). The gel is then displaced through this tear and that is what causes the displacement of disc. This is akin to the jelly leaking out of a jelly doughnut.
As noted above, disc herniations are always abnormal, always occur as a result of injury and require a tear in the disc lining. Disc injuries can occur when excessive mechanical forces are placed on the disc. These forces tear the annulus (disc lining) and then force disc material through the tear. Such forces are usually associated with flexion and stretching of the disc or with flexion and torsion (a twisting force) of the disc. This translates to a bending and twisting of the lower back while under a heavy load such as extreme flexion, positive or negative G forces, over twisting or all the above while carrying a heavy weight. Typical causes include unexpected high degree overloading, (such as in a car accident or a fall), repetitive fatigue from moderate overloading or improper techniques during sports or exercise.
Importantly, not every herniation is painful or painful to the degree that invasive treatments are required. Your doctor can determine based on your history, examination, MRI results and other tests if your disc herniation is causing problems. While herniations can heal or improve over time they can also worsen over time. An injury to the disc means that that disc can be re-subjected to injury with even less heavy loads as the original injury.
In addition to back pain a disc herniation can cause nerve pain. Nerve pain results from compression of the nerve or irritation of the nerve. If the herniation is sizeable, the disc material protrudes beyond its normal borders far enough to compress the nerves that travel behind the disc on the way out of the spine to serve the limb. Smaller herniations can irritate the nerves by causing inflammation that affects the nerves. The nerves can even become scarred and tethered to the disc. When nerve compression or irritation occurs you may develop nerve symptoms. The first symptom is pain radiating down the course of the nerve, down the leg. This is commonly called sciatica. The next worse symptom is numbness of the thigh, leg or foot. Lastly, if bad enough, nerve compression or irritation can cause limb weakness. This requires timely surgery for the best hopes of restoring limb function.
Symptoms
- Involves upper, mid or low back
- Constant aching back pain
- Pain radiating to buttocks, hips or thighs
- Pain may radiate to legs and feet
- May be associated with sciatica resulting in sharp and burning pain down thigh, leg or to feet.
- May be associated with numbness of thigh, leg or feet.
- May be associated with weakness of thigh, leg or feet.
- Back stiffness
- Painful sleep
- Pain with exertion or physical activity
- More pain with sitting than with standing
Signs
- Back muscle tenderness
- Diminished range of motion (difficulty with normal motion)
- Feeling of taught and tender knots in muscle
- Positive straight leg raise test: Lying on back and raising leg straightened at knee produces pain running down the leg. This results in stretching an already irritated spinal nerve.
- Numbness of thigh, leg or foot
- Diminished knee or ankle reflexes
- Weakness of the thigh, leg or foot
Diagnosis
A disc herniation is suspected when back pain persists beyond 6-8 weeks. Physical signs such as back tenderness, a straight leg raise test, numbness and weakness may be present. The next step will be an MRI to determine if there is a herniation and if so how many discs are affected. Your doctor will then determine if your symptoms are caused by the herniations seen on the MRI. If more than one herniation is present your doctor might order a discogram. A discogram is a test where dye is injected into a disc to determine if the disc has a tear and if that disc is causing pain. Lastly, an electromyogram (EMG) can be performed to evaluate nerve function. This is a test that measures the ability of a nerve to conduct an electrical current.
Treatment
- Conservative measures (Medications, therapy, activity restrictions, home exercises)
- Epidural injection if symptoms continue or are severe. This consists of an injection of an anesthetic and a powerful anti-inflammatory agent, called a steroid, into the spinal space surrounding the disc.
- Surgery may be warranted if symptoms are severe, persist or worsen. There are multiple forms of surgery. A discectomy is a procedure where the disc that has protruded through the tear in the disc lining is removed. In a fusion the disc is completely removed and replaced with bone. Most minimally invasive versions of this procedure are performed through a 22-millimeter opening.
- Endoscopic discectomy is a very minimally invasive option available today. The endoscope contains a camera and also an opening for surgical instruments. The endoscope allows the camera to be placed directly into the spine. As a result, a very small 7-millimeter opening is used and normal ligaments, muscle and bone usually do not have to be disrupted in order to treat the disc herniation. This operation is usually performed as an out-patient surgery and patients are up and about the same day.
The Degenerated Disc
Disc degeneration is a condition that occurs when there is deterioration or fatigue of one or more vertebral discs. This condition can develop as a natural part of the aging process or may also result from injury to the back.
Discussion
Doctors will often refer to “degenerative disc disease” when describing an abnormal disc that might be causing pain. However, even among doctors, the term is often misunderstood and is used in ways far different than intended. We’ll discuss two subtypes of “degenerative discs;” In one case a disc that has been subjected to the normal wear and tear of life (a normal aging disc) and in the other a disc that has been injured and develops a typical post injury appearance (a post-injury disc).
Normal wear and tear of the human joints begins early. The spine, consisting of joints joining vertebra together, is no exception. These changes can be seen on MRI. In some cases, these MRI changes can be seen as early as the teen years. In adulthood the changes become even more frequent. In fact, studies have shown that by middle to late adulthood these changes are almost universal. When MRI shows changes of normal wear and tear we don’t expect it to be associated with any symptoms. Studies have compared the MRI’s of patients with back pain and patients without back pain. Degenerative changes are just as frequent in both groups, meaning that they are common and don’t point to a specific cause of lower back pain.
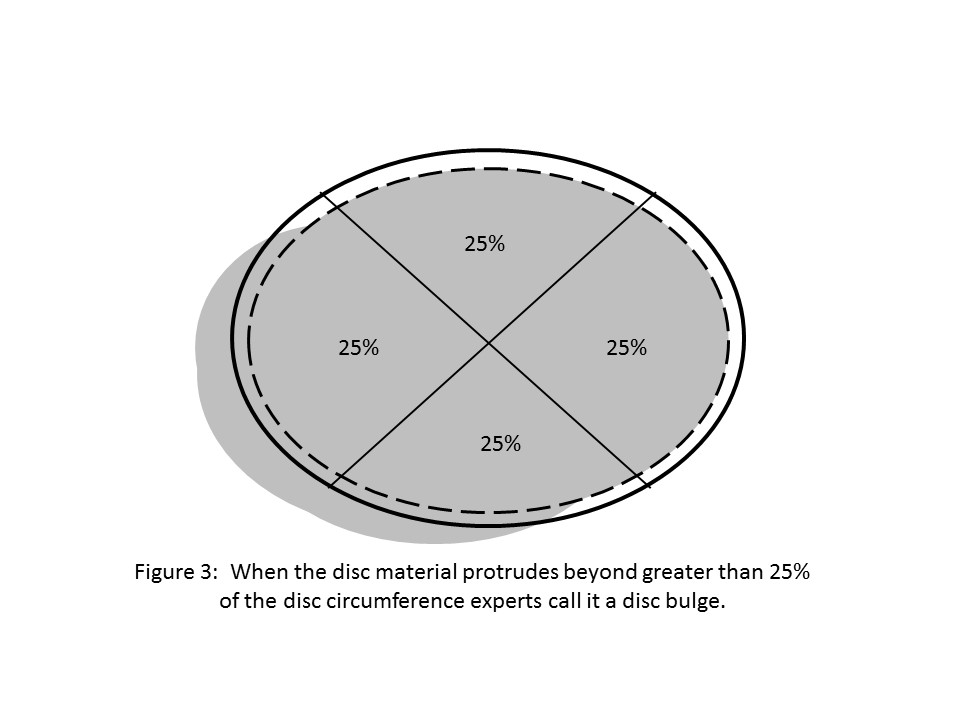
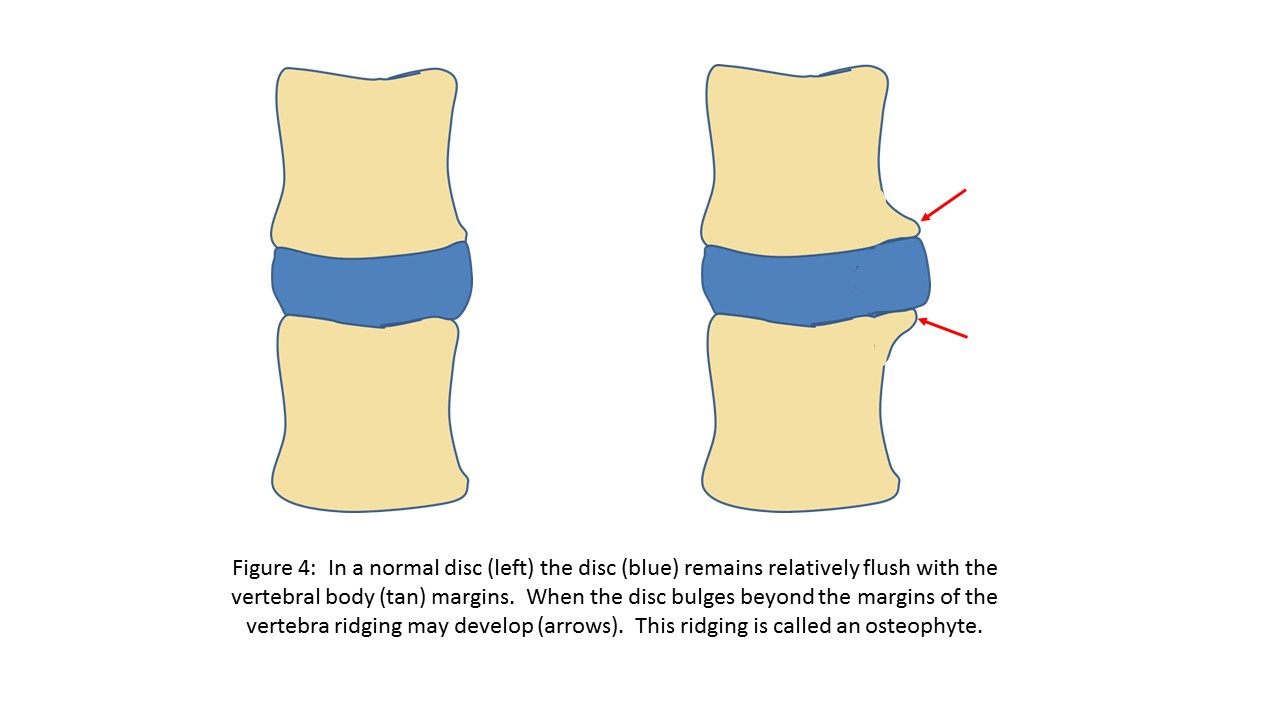
Normal wear and tear, or normal degeneration, has a very specific appearance on MRI. The disc itself has a diffuse bulge, meaning that greater than 25% of the disc circumference extends beyond the confines of the normal disc or the vertebra on either end of the disc (Figure 3). Since the bulging disc is attached to the vertebra, over time the bulging disc tugs at the bone, resulting in a bony protrusion or ridge, (called osteophyte), at the point of attachment of the disc to the bone (Figure 4). Another term for an osteophyte is “bony spur.” These changes are referred to as “spondylosis deformans” and are regarded by experts as a consequence of normal aging.
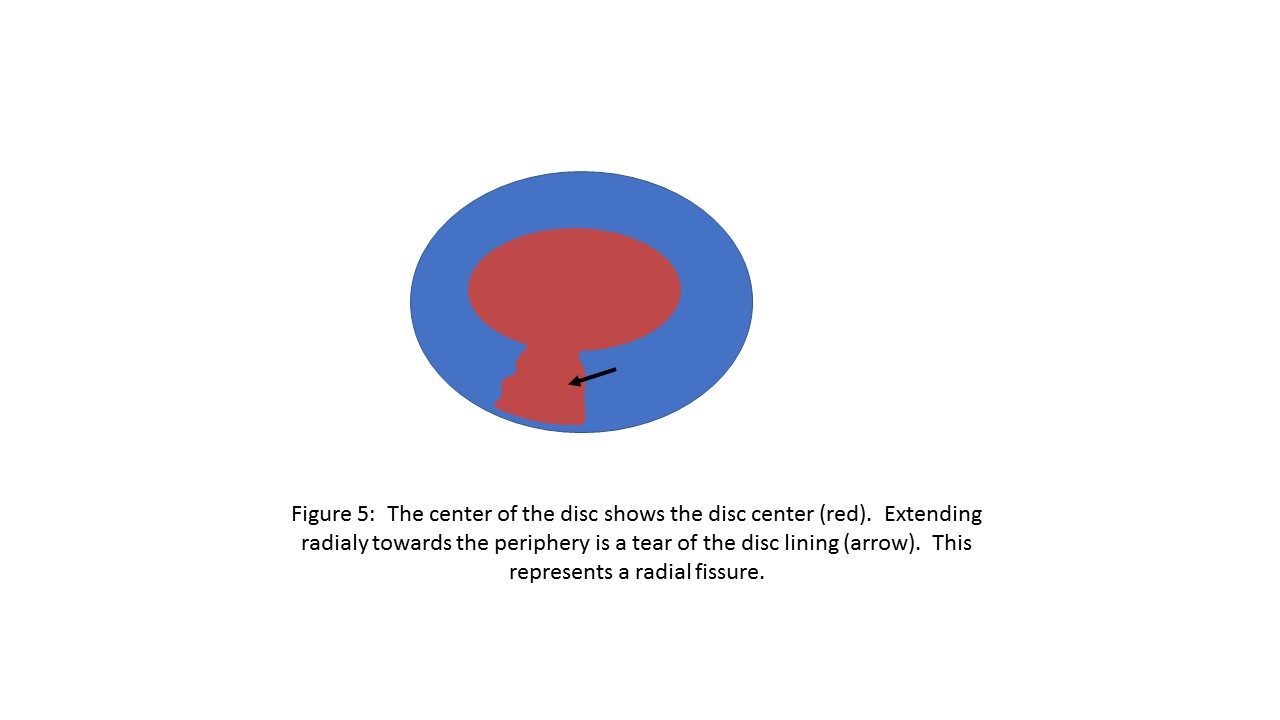
Fissuring is another type of disc degeneration. When the annulus, or disc lining, tears this is regarded as a fissure. Usually fissures are arranged radially from the disc center and are called radial fissures (Figure 5), extending towards the periphery. In some cases the fissures become so large that disc material travels into or through the fissure, causing a herniation (see above). Even when not resulting in a herniation a disc fissure can be quite painful and take some time to heal. These radial fissures are felt to be due to an injury of the disc, like the causes of disc herniation described above.
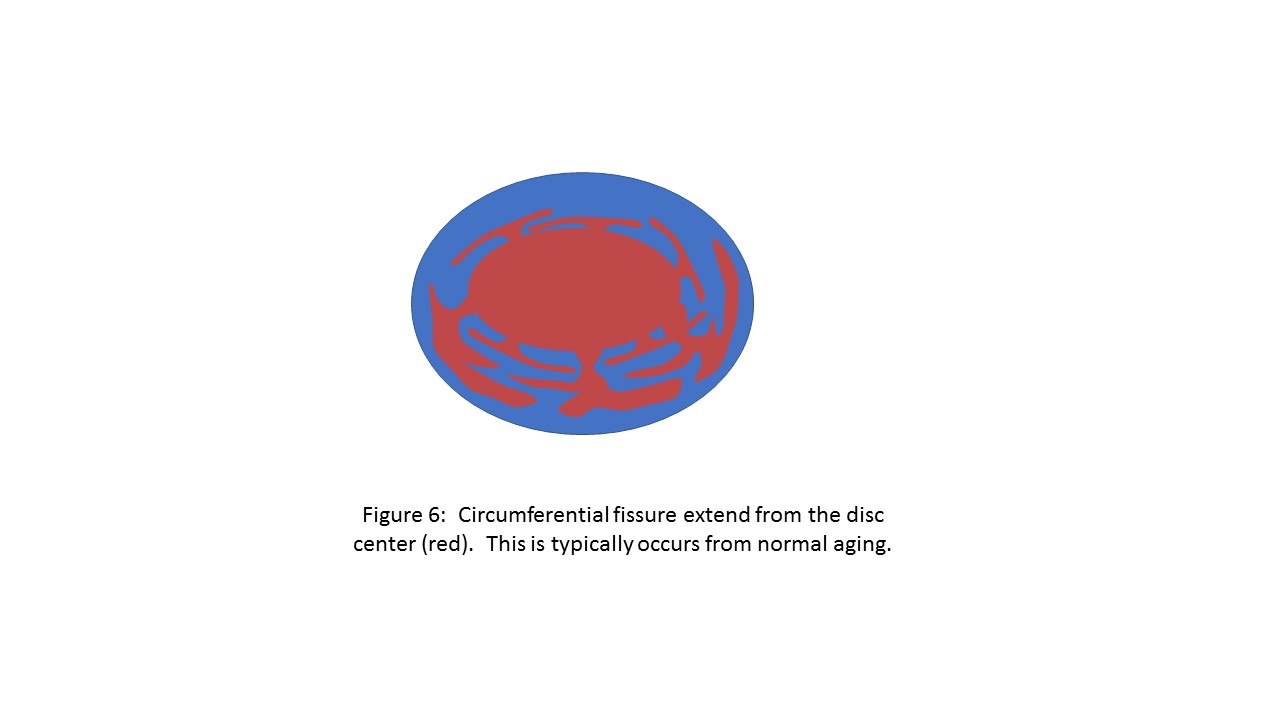
One type of fissure that probably does result from normal aging and doesn’t cause pain is circumferential fissuring (Figure 6). In circumferential fissuring the tears in the annulus are concentric and travel along the disc periphery, rather than out from its center, as the radial fissures do. When there are many circumferential fissures the disc is said to possess a “diffuse internal derangement.” Again, this does not imply that the disc is painful.
There are other degenerative changes that occur that are limited to the actual disc center. Desiccation refers to a loss of water content of the disc. On MRI water has a very specific appearance. As a disc degenerates it will dry, resulting in a change in MRI appearance from a wet disc to a dry disc. This likely results from a tear in the disc allowing water to escape. Desiccation is often accompanied by a loss of disc height. When seen, these are not the changes of normal aging. These degenerative changes have occurred because of injury to the disc at one time or another.
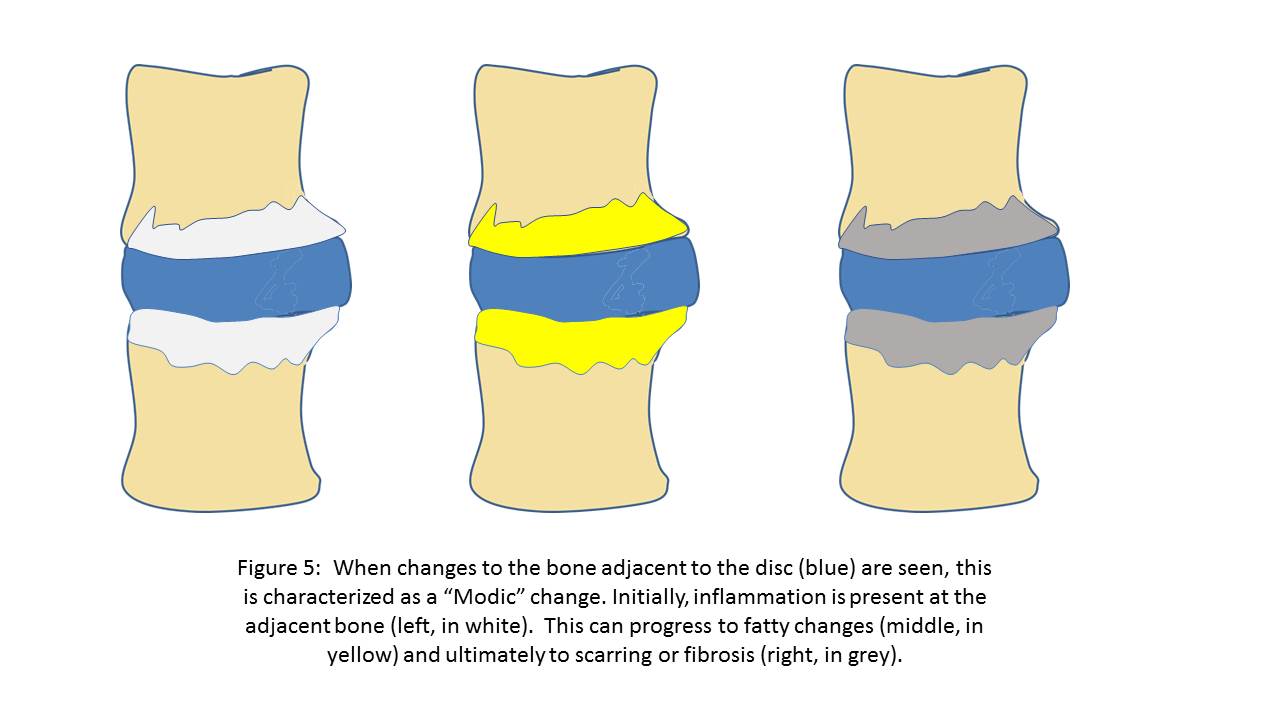
When a disc is injured and becomes degenerated one can see changes to the bone adjacent to the disc. Early on these changes will have the characteristic appearance of inflammation or swelling. Over time, these bony changes may transform to fat. Ultimately the bone becomes fibrotic, like scarring. Experts agree that inflammatory changes to the bone are often associated with back pain. Inflammation of the adjacent bone may be persistent or may “burn out” over time to become fatty or scarred. These changes are referred to by doctors as “Modic” changes, named after the doctor who first recognized them (Figure 7).
When degeneration has an appearance of normal aging, such as spondylosis deformans (osteophytes and disc bulging) or diffuse circumferential fissuring we don’t expect it to be associated with pain. The cause is normal wear and tear and it usually does not hurt. When degeneration has the appearance of radial fissures, disc desiccation, loss of disc height and Modic changes to the adjacent bone experts agree that there was likely an injury to the disc at one time or another. MRI cannot determine though whether these changes are painful. This requires a thoughtful evaluation of the patient.
Symptoms
- Degeneration from normal aging does not cause any symptoms
- Degeneration from injury may or may not cause the symptoms noted below:
- Upper, mid or low back
- Constant aching back pain
- Pain radiating to buttocks, hips or thighs
- Pain may radiate to legs and feet
- Sciatica resulting in sharp and burning pain down thigh, leg or to feet.
- Numbness of thigh, leg or feet.
- Weakness of thigh, leg or feet.
- Back stiffness
- Painful sleep
- Pain with exertion or physical activity
- More pain with sitting than with standing
Signs
- Degeneration from wear and tear is not associated with any signs.
- Degeneration from injury may or may not be associated with any signs.
- When post-injury degeneration results in symptoms all or some of the following signs may be present:
- Back muscle tenderness
- Diminished range of motion (difficulty with normal motion)
- Feeling of taught and tender knots in muscle
- When degeneration is associated with disc herniation the signs of disc herniation may be present (see above).
Diagnosis
The changes that encompass the term “disc degeneration” are identified on medical imaging. X-rays are able to show bony changes like osteophytes or bony spurs, fibrosis of bone and narrowing of discs. MRI can show the same findings as well as drying (desiccation) of the disc, changes to the adjacent bone and disc bulging. MRI might also show disc fissures.
When the MRI shows multiple discs with post-injury types of degeneration and the patient has symptoms of back pain the physician may order additional tests. A discogram is helpful in determining which disc is painful and is performed by having a physician gently inject dye into the disc to see if pain is provoked. A CT scan and x-rays can then be obtained, providing a detailed view of any fissures.
When degenerative changes occur after injury they may or may not be painful. To determine if the findings are associated with symptoms a careful history is taken and an examination is performed. These are not only the first but also the most important steps in determining the significance of degenerative changes on MRI. An MRI in and of itself does not tell us the presence of symptoms and one cannot determine the significance of the MRI findings without clinically evaluating the patient.
Treatment
- Normal age related degeneration requires no treatment.
- When injury related degeneration is present and is causing symptoms treatment is focused on addressing specific causes.
- Conservative measures can be undertaken for symptoms associated with post-injury degeneration (medications, therapy, activity restrictions, home exercises).
- Epidural injection is indicated for post injury symptoms associated with degeneration if symptoms continue or become severe despite conservative measures.
- Surgery may be indicated for post-injury symptoms associated with degeneration if symptoms are severe, persist or worsen. Surgery may be aimed at removing a herniation (discectomy), cauterizing a fissure (ablation or thermodiscoplasty) or replacing and removing the disc with either a prosthesis (disc replacement) or bone graft (fusion).
- Endoscopic surgery is a very minimally invasive option available today. The endoscope contains a camera and also an opening for surgical instruments. The endoscope allows the camera to be placed directly into the spine. As a result, a very small 7-millimeter opening is used and normal ligaments, muscle and bone usually do not have to be disrupted. Endoscopic surgery can now achieve many of the goals of traditional surgery.
Facet Joint Syndrome
The facet joints help stabilize the spine and limit excessive motion. Facet joint syndrome is caused by a deterioration or injury of the facet joints.
Discussion
The facet joints are vertically oriented joints located at the back of the vertebra. Each vertebra has a left and a right facet joint. The facet joint consists of the facet process (called articular process) of the vertebra above and below the joint. Like most joints, the facet joint is covered by a capsule. On the undersurface of the joint capsule there is a tissue called synovium which produces a lubricant that allows the joint surfaces to glide on each other. The inside of the joint is covered by a layer of cartilage. The joints allow flexion of the back and provides stability in extension, rotation and lateral bending. Injury can occur to any of the joint components; the bony facet process, joint capsule, cartilage or synovium.
The facet joints can cause back pain under several circumstances. The facet joint may become injured when repetitive and excessive forces are placed on the joint. This can occur in athletes or in individuals who perform heavy labor. A sudden and severe force can also cause injury. This can occur with a sudden hyper-extension of the back, as in a forceful push or an automobile collision. Lastly, a disc herniation or disc degeneration can cause undue stress on the facet joint. This occurs when a disc herniation or disc degeneration results in a loss of the normal cushion between vertebrae. This loss of cushion is compensated by increased stress being taken up by the fact joint. Since the fact joints are vertically oriented the loss of cushion causes an increased vertical sheer stress on the facet joint. Over time the facet joint may enlarge as it compensates for the increased stress.
Symptoms
- Mid and/or low back pain
- Pain radiates across back, to buttocks and thighs.
- Pain may radiate to legs
- Pain is aggravated by prolonged standing
- Pain is aggravated by lateral bending
- Pain is aggravated by twisting the back
- Pain is aggravated by changes in position like standing from a sitting position
- Pain improves with sitting or bending forward
Signs
- Pain upon pressing over the facet joints
- Diminished motion of the back
- Pain with extension of the back
- Pain with lateral bending of the back
Diagnosis
A facet injury is suspected when back pain lasts beyond 12 weeks, especially if it is worse with standing, extending, lateral bending or twisting. The diagnosis becomes highly suspected when MRI fails to identify a disc abnormality that may be resulting in the symptoms. MRI may or may not show abnormalities of the facet joint and cannot be relied upon to make the diagnosis of a painful facet joint.
A facet injection is useful for treating facet pain but is not as useful for diagnosing it. That’s because an injection inside the joint will spread to other areas of the spine, making the diagnosis non-specific. A medial branch block is a much more specific and accurate test to diagnose this condition. Here, a needle is precisely guided to the medial branch nerve, a branch of the spinal nerve that arises from the vertebral level. The medial branch provides sensation for the facet joint. “Blocking” the nerve means placing a small drop of anesthetic on it, much how a dentist blocks the nerves of the jaw before working on the lower teeth. The block can last for up to 5 hours, long enough for the physician to re-evaluate the patient and see if the signs and symptoms of facet joint pain have disappeared.
Treatment
- Conservative care measures such as rest, therapy and non-steroidal anti-inflammatory medications are used as first line treatment.
- Lumbar medial branch injection. This is used to definitively diagnose facet joint pain.
- Facet joint injection. This can last up to several months.
- Facet joint rhizotomy, or burning of the medial branch nerves that register facet joint pain. This can last up to 6 months.
- Extra-dural nerve avulsion. Here, the facet pain sensing medial branch nerve is identified using an endoscope placed through a tiny incision. An endoscope is a 7 millimeter tube with a high-resolution camera attached at its end. The medial branch nerve is cut allowing normal facet motion without pain. Because the procedure uses an endoscope it is minimally invasive and requires only a tiny incision. The procedure is usually permanent.
- Intervertebral fusion. Here the disc is replaced by bone and the vertebral segments are immobilized with screws and rods. Since there is no motion of the vertebral segment after fusion, facet joint pain is relieved.
- Endoscopic fusion is a minimally invasive way to achieve an intervertebral fusion. The endoscope contains a tiny high resolution camera placed directly into the spine. The endoscope also contains a port where tiny instruments are passed. The incision is small, usually about 10-millimeters and normal structures such as ligaments, bone and joints are preserved because of the smaller nature of the surgery. Otherwise, an endoscopic fusion is very similar to the traditional form of fusion described above.
- Facet joint fusion. A screw is placed across the joint so that it no longer moves. The lack of movement reduces pain generated by the facet joint.
Sacroiliac Joint Pain
The sacroiliac joint is an important joint between the pelvis and the lower spine. Sacroiliac joint pain is caused by degeneration or injury to the sacroiliac joint
The sacroiliac joint is the joint between the pelvis and the sacrum. The sacrum is the lowest part of the spine and ends in the tail bone. Like most joints, the sacroiliac joint has a capsule binding it together, synovium on the inside surface of the capsule that produces a lubricating fluid and cartilage on the inside surfaces. Unlike most joints there is not a lot of motion across a normal sacroiliac joint. Normal motion across this joint is only 2-18 degrees.
Sacroiliac joint pain is usually a result of repetitive abnormal stress on the joint. As a result, it typically occurs in older individuals. There are other conditions that can result in abnormal stress on the joint, leading to a painful degeneration. In women, multiple pregnancies can produce a lot of stress on the sacroiliac joint. Women with pregnancy-induced sacroiliac joint degeneration might develop symptoms in their 30’s and 40’s. Having had a low lumbar fusion, an operation where the 2 low lumbar vertebra are surgically joined, may also lead to sacroiliac joint pain. With a fusion one can no longer bend normally at the junction of the lumbar spine and sacrum. The sacroiliac joint will compensate by allowing more motion about the joint than it can normally accommodate. This can result in degeneration and intractable pain. Sacroiliac joint pain can also occur from an injury. A fall on the buttocks can cause a twisting motion at the pelvis, straining the joint. A car accident can cause a similar injury. If the foot is held firmly against the brake at impact force will be transmitted through the leg and into the hip, resulting in a twisting force at the sacroiliac joint.
Symptoms
- Low back pain
- Pain is localized to one or both sides of buttocks
- Pain may radiate to the thigh, hips or groin
- Pain may occasionally radiate down the leg
- Pain is worse with climbing stairs or lifting out of a chair
Signs
- The patient can place his/her finger across the sacroiliac joint when asked to localize pain
- There is tenderness when the sacroiliac joint is pressed upon
- There is increased pain when standing on one leg
- There is increased pain when the sacroiliac joint is examined using special physical examination manoeuvres designed to stress the joint
Diagnosis
Sacroiliac joint pain is suspected when there is low back pain and the MRI does not show a potential cause. In many cases previous attempts to treat back pain by targeting the disc or other joints have failed. When other causes of back pain have been excluded the physician should strongly consider the sacroiliac joint as the cause of pain.
In cases where the patient has had multiple pregnancies or there has been an L5/S1 fusion, sacroiliac joint pain should be considered early on as a potential cause of pain. These conditions, as discussed above, predispose to sacroiliac joint injury by causing a repetitive and abnormal stress on the joint.
Once sacroiliac joint pain is suspected the diagnosis is confirmed by physical examination. Physicians specializing in spine care are trained to perform several special sacroiliac joint examination maneuvers on a patient to evaluate for joint pain. These maneuvers and tests are called FABERS test, Gaenslen’s test, the compression test, the anterior superior iliac spine (ASIS) separation test and the active straight leg raise test. When most of these tests are positive there is a high probability that the sacroiliac joint is causing the patient’s pain.
Once there is a high index of suspicion the diagnosis is confirmed by performing a test called a sacroiliac joint block. In this test a small needle is advanced through the skin and into the affected joint. An anesthetic is then injected. The anesthetic will numb the joint for about 5 hours. During this time the physician can re-examine the joint. If pain is absent, one can reasonably conclude that the joint is the cause of the patient’s pain.
If one is considering a procedure to treat pain by coagulating the painful nerve endings of the sacroiliac joint (this procedure is called radiofrequency ablation) a diagnostic block is performed by injecting the pain sensing nerve endings of the joint. This block will predict the success of a radiofrequency ablation.
X-rays and MRI’s are rarely useful in the diagnosis of sacroiliac joint pain unless there has been a violent injury. Usually these studies will only show changes of wear and tear. Wear and tear in and of itself cannot predict if the joint is painful. Furthermore, a normal appearing joint can still be painful.
Treatment
- Conservative measures like medications, exercise and therapy are first line treatment options.
- For persistent pain, sacroiliac joint injections are performed using anesthetic drugs and powerful anti-inflammatory medications called steroids. The results can last 2-3 months, or more.
- In some cases a radiofrequency ablation can be performed to treat sacroiliac joint pain. Here the nerves that sense pain signals from the sacroiliac joint are interrupted by coagulating those nerves using a special needle and energy. The procedure may last several months or more.
- A potentially permanent fix is a fusion across the sacroiliac joint. This is achieved by using a small incision and placing small screws across the joint.
Spinal Stenosis
The spinal column contains open spaces that create passageways for the spinal cord and the spinal nerves. Spinal stenosis is a narrowing of (or an intrusion into) these openings. This can cause a compression of the nerves.
Discussion
Spinal stenosis can effect several different nerve passageways of the spine. When the central part of the spine is affected this is called central stenosis. This affects the nerves traveling up and down the spine. When the passageways where nerves preparing to exit or exiting the spine are affected this is called foraminal stenosis and lateral recess stenosis. This narrowing is detected on MRI or CT scans of the spine. To be clinically meaningful, stenosis must be associated with symptoms attributable to the narrowing seen on imaging.
Stenosis usually occurs because of degeneration of the spine. When the disc degenerates it can bulge outwards or sideways, intruding into the passageways of the spine. Another form of degeneration is hypertrophy. Hypertrophy occurs when a bone or a ligament is under undue stress. Like muscle, the bone or the ligament will enlarge in order to cope with the physical stress. This is called hypertrophy. Hypertrophy of the facet joints and a major ligament in the back of the spine, (the ligamentum flavum), can cause stenosis by impinging on the nerves as they travel through the spinal canal. Oftentimes stenosis results from a combination of all of these factors.
Stenosis can sometimes worsen or improve based on posture. When one is standing the spine is in extension, or bent slightly back. This posture will narrow the nerve pathways of the spine. This places pressure on nerves resulting in buttocks, thigh or leg pain. Bending forward, or sitting, places the spine in flexion. This posture enlarges the spinal passageways. This can relieve the symptoms of nerve compression. Changes in symptoms with posture can be a clue to the presence of stenosis. The diagnosis is suspected when patients experience radiating leg pain when standing or walking, only to have the symptoms rapidly improve when bending forward or sitting.
Symptoms
- Radiating buttocks, thigh or leg pain with standing
- Resolution or improvement of symptoms with bending forward or sitting
- May or may not be associated with low back pain
- May or may not be associated with numbness
- May or may not be associated with weakness
Signs
- Detectable loss of sensation in lower extremities
- Detectable weakness in lower extremities
- Palpable tenderness to low back
Diagnosis
Spinal stenosis is considered both a clinical syndrome and a radiological diagnosis. Clinical syndrome means that there are a particular set of symptoms that the patient is experiencing, as described above. Commonly, patients suffering from spinal stenosis will complain of buttocks, thigh and leg pain that appears or worsens with standing or walking. This should clue the physician to the possibility of spinal stenosis. Spinal stenosis is also a radiological diagnosis, meaning that MRI and CT has detected areas of the spine where there is narrowing of nerve passageways. When a patient has imaging findings of spinal stenosis and possesses symptoms ascribable to the narrowing seen on MRI and CT the diagnosis is confirmed.
Once a careful medical evaluation and medical imaging makes the diagnosis of spinal stenosis additional tests can be performed to determine the severity of nerve compression. This involves performing an electromyogram (EMG). This is a test where needles are used to measure the electrical conduction between muscles and nerves. EMG is not always necessary if the diagnosis is obvious.
It’s important to note that stenosis on medical imaging without the clinical syndrome is meaningless. In other words, stenosis seen on MRI or CT scans does not have to be treated if there are no symptoms of pain, numbness or weakness.
Treatment
- Conservative measures like medications, exercise and therapy are first line treatment options.
- Epidural injections can provide temporary relief when conservative measures don’t work
- Traditional surgery for persistent cases involves opening the passageways where the nerves travel in the spine, to relieve pressure. This is called a laminectomy. This is sometimes combined with a fusion procedure, where the disc is replaced with a prosthesis and bone. These days the procedure is performed through a 22-millimeter tube.
- Endoscopic decompression is a minimally invasive form of laminotomy, or opening of the main channel in the spine. Because the endoscope is a camera placed directly into the spine a smaller opening is used, as small as 10-millimeters.
- A minimally invasive option that recently became FDA approved is the Superion Interspinous Spacer. This acts like a “jack” to keep the spinal passageways open when standing and walking.
Spondylolisthesis
Spondylolisthesis occurs when a lumbar vertebra slips out of place. The slippage may cause back pain or may irritate the nerves of the spine.
Discussion
Spondylolisthesis is a medical term that describes the slippage of a vertebra relative to the normal spine. Normally the vertebra are aligned with one another so that there is a smooth curve from the top of the spine to the bottom. With spondylolisthesis, sometimes just called listhesis, the normal curve is disrupted by a forward or backwards slip of the vertebra. The slip may be mild, moderate or severe. Severity of the slip is measured by the amount of slippage. When there is associated degeneration of the facet joints or bulging discs a mild slip can cause compression of the nerve passageways. Otherwise, a moderate or severe slippage is required to compress the nerve passageways. The slippage may also be stable or unstable. A slip is said to be stable if the degree of slippage does not change with bending forwards or backwards. A slip is unstable if there is increased slippage with bending forwards and backwards. An unstable slip will often cause back pain and may cause nerve pain by compressing nerve passageways.
There are multiple causes of spondylolisthesis. In young people it can occur because of a birth defect in part of the vertebra. Some people, usually young competitive athletes, can develop a spondylolisthesis from over stressing the spine and causing a type of fracture of the vertebra called a stress fracture. This occurs in about 6% of the general population. This type of spondylolisthesis is referred to as “spondylolysis.” The “-lysis” at the end denotes that the cause is a defect in the bone of the pars, (the part of a vertebra that joins with the vertebra above and below it). When spondylo-“lysis” causes a slippage of the vertebra the condition for spondylo-“listhesis” is met. “-listhesis” means that there has been a slippage. When spondylolysis and spondylolisthesis exist the condition is not necessarily painful. In fact, subjects with spondylolysis and spondylolisthesis have the same rate of lower back pain as the rest of the population.
Another common cause of spondylolisthesis is degeneration of the spine. Stability, or the ability of the spine to resist abnormal movement and forces, is dependent on the spinal muscles, spinal ligaments, facet joints (the joints that join the back of the vertebra to each other) and the discs. Degeneration of the discs can lead to added stress on the facet joints and the lining of the disc (the annulus), which attach to the vertebra above and below. Over time the disc and the facet joints of the spine can degenerate so greatly that laxity develops. This laxity can become so great that normal forces placed on the spine can overcome the ability of the disc and joints to resist those forces. As a result spondylolisthesis develops. This type of spondylolisthesis is called degenerative spondylolisthesis. Degenerative spondylolisthesis may or may not be painful.
Spondylolisthesis may rarely be caused by more dangerous conditions. Infection, tumor and fractures can all result in spondylolisthesis. Fortunately, these underlying conditions can often be readily diagnosed on MRI.
Symptoms
- Spondylolisthesis may not be associated with any symptoms at all
- When spondylolisthesis results in symptoms all or some of the following signs may be present:
- Back muscle tenderness
- Diminished range of motion (difficulty with normal motion)
- Feeling of taught and tender knots in muscle
- Pain across the lower back
- Pain radiating to the hips, buttocks, thighs or leg
- Pain with bending
- When spondylolisthesis causes nerve compression the following symptoms may be present
- Burning pain radiating down the thigh or leg
- Burning pain reaching the foot
- Numbness of the thigh, leg and foot
- Weakness of the leg
Signs
- Pain and tenderness may be present on palpation of the spine and facet joints
- Pressure placed on the bony prominences of a vertebra may result in motion
- Pain may be present with flexion or extension of the back
- Loss of neurological function might be detected on examination, such as numbness or weakness
Diagnosis
Spondylolisthesis is a radiographic diagnosis, meaning that it is diagnosed by viewing x-rays, CT or MRI of the spine. X-ray is a convenient test to study the alignment of the bones and will usually diagnose a spondylolisthesis. X-ray can also be performed with bending or extending and can be used to determine if spondylolisthesis is stable or not. If the listhesis increases with motion it is felt to be unstable. To determine if the slippage is from spondylolysis (congenital defect or stress fracture) vs. a degenerative process further studies are required. CT has excellent definition of bones and is superior for detecting the congenital defects and stress fractures associated with spondylolysis. MRI is very useful for the detection of degenerative spondylolisthesis as it can easily show the degenerative facet joint and discs associated with the condition. Also, MRI allows visualization of the nerves as they pass through the spinal passageways. This allows the physician or the surgeon to determine if nerve compression is present.
Symptoms from spondylolisthesis can come from various sources, not necessarily just the slippage itself. If the spondylolisthesis is causing compression of the nerves then nerve pain may arise. This can be diagnosed by injecting the compressed nerve with an anesthetic agent to see if the pain disappears. This is called a nerve block. The joints of the spine can be overly stressed in degenerative spondylolisthesis. This is diagnosed by injecting the joints with an anesthetic. This is called a facet block. The disc may also be a source of pain. A discogram is a procedure where the disc is injected to see if pain is provoked. Lastly, pain may come from the bony defect in the stress fracture form of spondylolysis. The defect can be injected with an anesthetic to see if pain is relieved.
While spondylolisthesis is a radiographical diagnosis, x-rays, CT and MRI cannot determine if the spondylolisthesis is causing symptoms or not. This requires a careful medical evaluation and physical examination. Treatment would only be recommended for symptomatic cases.
Treatment
- Conservative measures like medications, exercise and therapy are considered first line.
- Facet injections may relieve pain for up to 2-3 months in some cases.
- Nerve blocks or epidural injections can reduce symptoms from nerve compression for up to several months.
- Decompressive surgery can open the compressed spaces of the nerves if the spondylolisthesis is stable and if done minimally invasively.
- Painful and unstable spondylolisthesis may require fusion. In fusion the disc is removed and replaced with bone. Stability is provided with the use of screws and rods.
- Endoscopic fusion is a minimally invasive way to achieve an intervertebral fusion. The endoscope contains a tiny high resolution camera placed directly into the spine. The endoscope also contains a port where tiny instruments are passed. The incision is small, usually about 10-millimeters. This allows normal structures such as ligaments, bone and joints to be preserved because of the smaller nature of the surgery.
- Stable spondylolisthesis with pain attributable to the disc may be treated with minimally invasive procedures that treat the degenerated disc. One example is endoscopic discectomy.
- Asymptomatic spondylolisthesis requires no treatment.
Failed Back Surgery Syndrome
Failed back surgery syndrome occurs when there is persistent pain after back surgery. There are several potential causes for failed back surgery syndrome.
Discussion
Failed back surgery syndrome occurs when a patient has had surgery, yet symptoms persist and surgery is deemed unsuccessful. There are many reasons why surgery could be perceived as being unsuccessful. The most common cause of out-right surgical failure is inadequately addressing the main or major cause of pain. This can occur if not all painful disc levels are treated or if surgery does not adequately relieve the pressure on a compressed nerve.
Another cause of failed surgery is due to a consequence of surgery, even though the initial procedure was successful. In some individuals significant scarring may take place inside the spine over a period of 6-12 months after surgery. This can inflame nerves and result in a return of pain. This is suspected when there is a return of nerve systems and an MRI only shows post-surgical scarring. Other examples can be seen after fusion surgery. After a successful fusion there is a limitation in the normal motion of the spine. This can over-stress the spinal segments above or below the fusion segment. This can lead to a subsequent herniation of the over-stressed segment and can be seen in up to 20% of cases. The symptoms can be identical to the symptoms necessitating the original surgery. Another cause is a failure of the fusion. In this case, the expected solid bone formation bridging the vertebra above and below an operated-on disc level never takes place. The resultant motion between the 2 vertebra can be painful. This can occur in up to 10% of cases, necessitating a re-fusion. Again, the symptoms can be very similar to the original pre-surgical symptoms.
A return of symptoms for reasons unrelated to the initial procedure can also be seen. One example is when the patient’s pain syndrome changes over time. This can be seen when a degenerative arthritis occurs as a consequence of the initial injury. The patient can usually discern that these symptoms are somewhat different than the initial symptoms prior to surgery. Another cause is leftover pain after surgery that is less intense than the pain before surgery. This can be an indication that there may be another contributor to pain. For example, a discectomy may relieve pain from sciatica or disc herniation but the patient may also be having pain from the facet joints behind the disc or the sacroiliac joints that join the pelvis and sacrum together. After treating the major pain generator, the leftover pain may now become a major focus for the patient. Careful diagnostic testing can determine the cause of the leftover pain. Finally, a cause of a return of symptoms can be a return of the previous condition, but at another level. This is usually seen as a herniated disc or a vertebral fracture at a level other than the originally operated on level.
Persistent symptoms may also represent a harbinger of a complication of surgery. This includes disc inflammation (discitis) or full blown infection of the spinal discs and bones. MRI is essential in making this diagnosis. Another complication, injuring a nerve in surgery, can also cause chronic pain that can be worse than the pain leading to surgery in the first place. In these cases, one might initially note weakness or numbness right after surgery in the limb affected by the injured nerve.
A recurrence of disc herniation after surgery is not so much a failure of surgery as much as a limitation in the durability of surgery. After an injury to the disc lining, or annulus, the disc will be susceptible to re-injury. When this occurs after surgery it is called a re-herniation. Under normal conditions the re-herniation rate is 6%-7% after a discectomy. Re-herniation is usually treated by conservative measures. If those fail a reoperation may be necessary.
Patient expectations may also contribute to a perception of failed back surgery. In some cases a patient’s expectations of success are unrealistic. It should be explained that the goal of surgery is not to relieve all pain. The goal of surgery is to relieve pain sufficiently that the patient has reduced disability and can adequately increase their activity to a desired level. Proper counselling before and after surgery can insure that patients have realistic expectations with which to judge their results.
Lastly, in some cases, surgery prematurely perceived as being unsuccessful when in fact it really was. This can occur when too little time has passed to allow healing at the surgical sight. Generally speaking, one should allow up to 3 months before making a determination on the success of surgery. Once healing and surgical side effects have worn off the patient may indeed experience significant relief.
Symptoms
- Back pain radiating to hips, buttocks or thighs
- Radiating thigh, leg and foot pain
- Numbness of the thigh, leg or foot
- Limb weakness
- Symptoms may be similar or different than prior to surgery
- In cases of infection, malaise and chills may be present
Signs
- Limb weakness on examination
- Spinal tenderness
- Diminished limb sensation
- Fever and abnormal laboratory studies are seen in cases of infection
Diagnosis
As discussed above, a truly failed back surgery should be distinguished from an effective surgery with recurrent or residual pain due to another cause. Careful evaluation of the patient by an experienced physician can usually determine if residual or recurrent pain is due to a complication, unrealistic expectations, a residual pain generator not addressed by surgery or a new pain generator that has occurred over time. Diagnostic testing, including MRI, blood tests and injections may be necessary to completely evaluate the new, recurrent or persistent symptoms. Importantly, the patient must remain patient as the physician diligently seeks to explain the post-surgery symptoms. In many cases the answer to what is causing the symptoms will not be obvious and will not be easily uncovered. However, a careful evaluation will ultimately reveal the cause. Simply labelling a patient as having “failed” surgery is inadequate and is no substitute for arriving at a precise diagnosis. The exception is scarring leading to nerve symptoms. This is usually a diagnosis of exclusion, meaning that a careful evaluation has ruled out all other causes.
Treatment
- Appropriate counselling can avoid a diagnosis of failed back surgery syndrome in cases where the patient may have unreasonable expectations, minor residual pain from another source or pain from a new source.
- Pain related to surgical side effects can be treated with medications and, if necessary, spinal injections such as epidural injections and facet injections.
- A complication from surgery leading to significant and disproportionate pain should be treated expeditiously.
- If re-operation is required to address an un-treated or under-treated condition the surgeon must take great care to ascertain that the correct diagnosis has been reached and that the proposed procedure will address the condition. This may require additional diagnostic tests and spinal injections to pin-point the cause of pain.
- A spinal cord stimulator may be helpful in treating failed back surgery syndrome. A stimulator stimulates the spinal cord or nerves by transmitting an electrical signal, thereby blocking the perception of pain. A stimulator is indicated in a variety of conditions including where it is felt that nerve irritating scar has formed in the spine, there has been permanent nerve injury after surgery or where the patient does not wish another surgery for a residual or unrelated condition.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}